Another clue for Chagas was that
In April 1908 Chagas spent the night in a house where he found a sickly cat, which he examined, finding T.
Rita had a fever of 40°C (105°F) for two weeks. Her spleen and liver were enlarged and her lymph nodes were swollen. Most noticeable to Chagas was a generalized infiltration, more pronounced in the face, and which did not show the characteristics of renal edema but rather of myxedema. Carlos Chagas (1911) found this last symptom to be one of the most characteristic forms of the acute stage of the disease; it revealed some functional alteration of the thyroid gland, perhaps affected by the pathogenic action of the parasite.
Three days later, Rita died from parasitemia caused by

The pathology of Chagas’ disease varies from a mild and inapparent infection as was found in Bernice, who outlived Carlos Chagas by twenty-seven years, to Rita, the three-year-old girl who died from a virulent acute infection. Because its pathology varies so widely, the diagnosis of Chagas’ disease from symptoms is difficult.
Animal studies were needed by Chagas to claim that
The journey from Lassance was a grueling twenty-four-hour trip, with two train changes and long waits. Chagas and Cruz knew that this discovery would place them, the Institute Oswaldo Cruz, and Brazil in the forefront of tropical medicine throughout the world. Cruz met Chagas at the railroad station and took him directly to the laboratory, where the mammalian pathogenicity of the flagellate was confirmed.
Carlos Chagas and Oswaldo Cruz later proved that
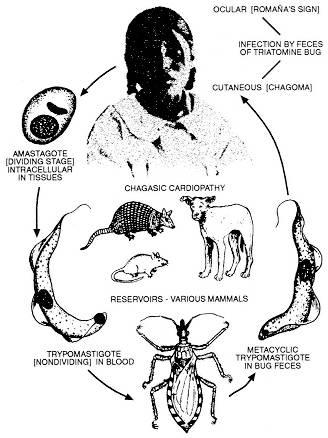
Progression of Chagas’ Disease
Carlos Chagas discovered the symptoms and progression of Chagas’ disease. Figure 8 illustrates how Chagas’ disease progresses, which is a complex and in part unresolved issue. Primary Chagas’ disease refers to the acute infection stage, which may not be clinically apparent, with about 25 percent of infected patients indicating it (see Appendix 9). If apparent, it is characterized by inflammation that may include fever, general malaise, swelling and soreness of the lymph nodes and spleen, and by
Infected victims pass into early latent Chagas’, which is asymptomatic. Latent Chagas’ offers several possibilities: 1) the infection is arrested at this stage, 2) it develops later to late latent Chagas’ with minor clinical findings, or 3) it develops into classic chronic (tertiary) Chagas’ disease. Those with minor clinical findings progress to either early latent arrested (secondary) Chagas’ or classic chronic (tertiary) Chagas’.
A certain number of patients live out their lives in the early latent arrested phase, with no noticeable symptoms, except perhaps fatigue. As mentioned, one acute patient of Carlos Chagas in 1909, Bernice, lived past the age of seventy and was checked annually, with no symptoms of the disease ever being manifested (Lewinsohn 1979:519). However, in many instances, the disease culminates with classic chronic symptoms of tertiary Chagas’heart disease and enlarged colon and esophaguswhich if untreated result in death. There is no known cure for the chronic phase.
Chagas’ disease is closely related to the immune system. Its progression varies greatly with the immunocompetence of each individual. Bolivians suffer so greatly from it in part because many are malnourished and infected with other diseases (see Appendix II).
At the Brazilian National Academy of Medicine’s session on April 22, 1909, Oswaldo Cruz read Chagas’ work entitled “A New Human Trypanosomiasis.” Cruz referred to the new disease as American trypanosomiasis to distinguish it from African trypanosomiasis, but American trypanosomiasis was soon known as Chagas’ disease (Kean 1977). Shortly after the reading of the paper, Cruz and a group of distinguished physicians traveled to Lassance to visit Chagas at work. Miguel Couto described the visit:
Carlos Chagas was waiting for us with his museum of laboratory items. Examination between cover-glass and slide revealed the raritiesseveral dozen patients of all ages, some idiots, others paralytics, others heart cases, thyroids, myxedemics and asthenics. Microscopes were scattered all over the tables showing trypanosomes in movement, or pathological anatomic lesions. In the cases were animals experimentally infected and jars full of